 Contact Us
Contact Us
 Join Us
Join Us
 Member Login
Member Login
 Create eAccount
Create eAccount
-
ROOT OF HONG KONG MIDWIFERY
By Anne WM Chow from HKJGOM 2000 ; 1 : 72-80
The history of midwifery in Hong Kong can be traced back to pre-colonial days. At that time, women had their confinements at home attended by their own female relatives or the traditional Chinese midwives called "Wan Po" (隱婆). These "Wan Po" were a group of "wise" women who had virtually no formal education. Their knowledge in midwifery was acquired through their own experience or attending others during childbirth. The knowledge passed from one generation to the next through verbal instruction. The "Wan Pos" knew nothing about asepsis. Septicaemia contributed a major cause of maternal and infant mortalities.
Even though Western medicine was introduced to Hong Kong in late 19th Century, the local Chinese still preferred Traditional Chinese Medicine. There was no maternity hospital, but on and off, a number of midwifery cases were reported in the general hospitals. Home confinement was the norm as Chinese women would not accept a male doctor attending their deliveries. In 1897, a maternity block was added as an annexe to the Government Civil Hospital. There were 20 confinements for that year. The maternal mortality at that time was high. In the Report of the Medical Officer of Health for Hong Kong for the year 1900, it stated that "......from the mortality returns no less than forty young Chinese women succumbed to disease incidental to childbirth during the year.....". In 1901, Dr. Gibson of Nethersole Hospital reported that out of the 15 midwifery cases admitted to the hospital, 4 had died, "... the women having been treated before arrival by (traditional) Chinese midwives, and were moribund on arrival'.
The first maternity hospital, Alice Memorial Maternity Hospital, was opened on 7th June 1904 under the charge of Dr. Sibree who came from London Missionary Society. Dr. Sibree was the lady doctor whom the local community had been long waited for. She commenced the formal training of midwives in the same year. It was a two-year course based on the British curriculum. The student midwives had to complete the general nursing training before being admitted to this program. Three student midwives were recruited. They passed the first Government examination for midwives held in 1906 and received the certificate of qualification. Examiners were doctors and one of them was the Hon. Dr. Ho Kai. The practice of having solely doctors as examiners had not changed until the revision of Midwives Registration Ordinance in 1999.
In 1905, the Government Maternity Hospital sent their midwives to the Alice Memorial Maternity Hospital for training. Since then, the local Chinese gradually accepted delivery of babies by western method though women were still reluctant to have hospital confinement. As such, Dr. Sibree and her team of eight Government midwives took their maternity services to the women's homes. In 1909, they had done 1381 domiciliary deliveries while there were only 235 hospital confinements.
-
1910 - 1941
PRE WAR ERA OF TRANSFORMATION
The growing acceptance of the western method of delivery of babies had led to insufficient maternity beds in the hospital and great demand for trained midwives. This had an impact on the training of midwives and brought about changes in the training system. According to the Register of Midwives of Hong Kong Midwives Board, there existed two midwifery training programs as early as 1911: one for registered nurses which was a one-year course and the other was a two-year program for those without nursing qualification, i.e. the "direct entry" midwives. The Alice Memorial Maternity Hospital was the training center at that time.
The Establishment of Statutory Governing Body
The commencement of training and the birth of a profession necessitated the formation of a statutory body for the control and monitoring of professional practice. In 1910, the Hong Kong Midwives Board was established under the auspices of the Midwives Registration Ordinance No.22. It is a statutory body which governs the training and examination of midwives, their registration and practice. The Board was empowered to register or deregister any appropriate person, and to maintain a roll of midwives. After 1912 “No one shall habitually and for a gain attend women in childbirth unless she be certified by the Board”. In spite of the Ordinance, ‘Wan Pos’ were still practicing in remote villages and neglected slums. In 1937, 111 ‘Wan Pos’ who had practiced midwifery in Hong Kong for tow or more years were enrolled as midwives following a short in-service training.The Growing Demand in Midwifery Training
In view of increasing demand for midwives, midwifery schools were set up one after another. In 1920, Government Civil Hospital began to conduct midwifery training. Tsan Yuk Hospital was opened in 1922 to provide maternity services and to train Chinese midwives. Six student midwives were recruited and they graduated in 1925. The Tung Wah Groups of Hospital, the three hospitals that were established to meet the needs of the local Chinese, also commenced western midwifery training, viz. Kwong Wah Hospital started the training in 1925 with Tung Wah Hospital and Tung Wah Eastern Hospital in 1930 and 1932 respectively. Training of midwives in private hospitals started in 1934 at the Hong Kong Sanatorium and Hospital. The teachers were obstetricians and senior midwifery sister on the maternity wards. -
THE FORMATION OF PROFESSIONAL BODY

The Hong Kong Nurses and Midwives Association was founded in 1940 with the objectives of maintaining the standard of nursing care, promoting unity among nurse/midwife colleagues and protecting the interest of the nurses and midwives. The association organized courses for its members and also engaged in activities that would improve the maternity service.
In 1940, the Midwives Board announced that midwives who had graduated for more than seven years had to take a four weeks full time refresher course in an appointed hospital. During this 4 weeks, they were forbidden to practise as a midwife. In addition, they had to pay the course and accommodation fee to the hospital. This proposal was strongly opposed by the practicing midwives as their livelihood would somehow be affected. Acting on their behalf, the representatives of the Hong Kong Nurses and Midwives Association negotiated with the Midwives Board. Finally, with the help of Professor Gordon King, the Chair of the
Department of Obstetrics and Gynaecology of the Hong Kong University, it was agreed that exemption would be granted to midwives aged over 50 or those not currently practising midwifery.Independent Role of Midwives
In these early days, midwives worked as an independent practitioner. Their main responsibility was to attend women at birth, either at the woman's home or in hospitals. Doctor would be called only when abnormality was detected. In fact, from 1913 to 1919, maternity services at the Alice Memorial Maternity Hospital was maintained mainly by midwives since there was no doctor to head the service. However, their role in antenatal care was minimal. It was because pregnant women at that time seldom came back for antenatal check up despite they were encouraged to attend the newly established antenatal clinic. According to the records, Alice Memorial Maternity Hospital had only 50 to 100 sporadic antenatal attendances a year. Tsan Yuk Hospital had similar experience when the antenatal clinic was established in 1929.
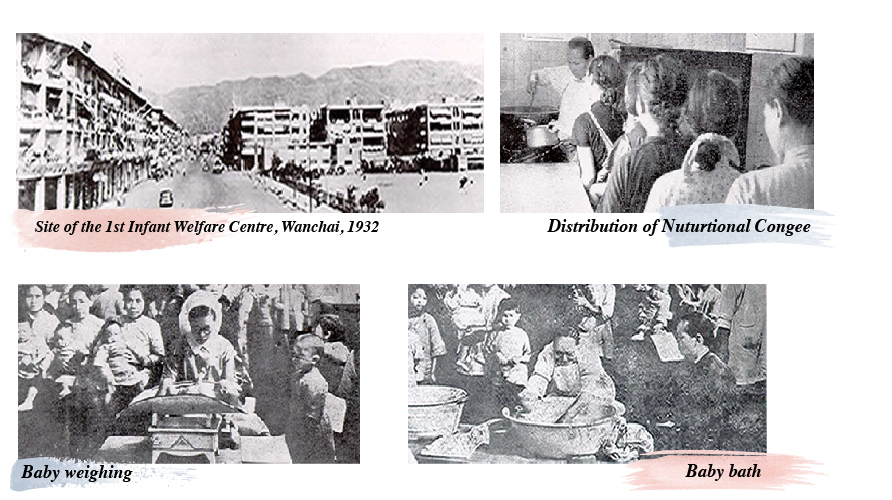
Hong Kong was, by then, still under-developed and the infant mortality was very high. Only about half of the babies born survived their first year of life. Malnutrition and gastro-intestinal disturbance were the common problems. For this reason, the first Government "Infant Welfare Centre" was set up in 1932 to look after babies and provide health education to young mothers on infant care. Midwives conducted morning talks to mothers and demonstrated baby bath. They also spent much of their time on one-to-one instruction on proper infant feeding techniques. In 1934, the practice of providing free nutritional congee to poor nursing mothers and under-nourished older babies started. This was a great boon for the poor people to come to the centres, and did much to improve the health of the mothers and babies.
-
1945 - 1960s
POST WAR ERA OF EXPANSION
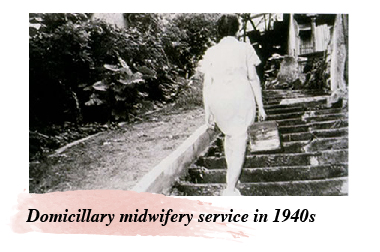
After the World War II, Hong Kong was in a state of material shortage. Despite hospitals were reopened, pregnant women still preferred to have home delivery or birth at a small, midwife-led unit called maternity home. To meet the demand, seven maternity homes and six domiciliary centres were opened in 1946 in different areas of Hong Kong. The post-war period was also a time of baby boom. The birth rate in 1950 to 1956 was at a record high of 34.0 to 37.0 per 1000 population. From 1958 to 1965, the number of deliveries in Hong Kong exceeded 10,000 per year. In 1950s, political uncertainty in Mainland China caused an influx of immigrants to Hong Kong. This resulted in a rapid rise in population leading to problems in housing, water supply and sanitation. Infectious diseases were very common. The poor living condition discourage home births. At that time, home birth accounted only for about 2-3% of the total births. Deliveries took place either in hospitals (about 50%) or maternity homes (approximately 47%). This caused severe overcrowding in the maternity units. As one retired midwife recollected, two women sharing the same bed was a common scene on the maternity wards. In 1958, Tsan Yuk Hospital had to restrict the booking to only those high risk pregnant women. The normal cases including primigravidae would have deliveries at maternity homes while pregnant women with abnormalities or complications would be cared in hospitals.
The Inception of Maternal and Child Health Centres
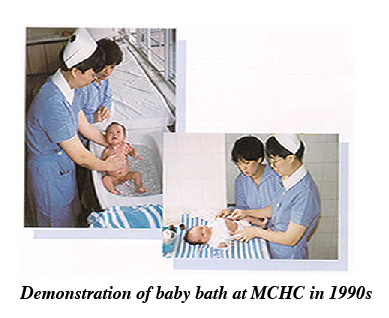
To meet the increasing demand, new Maternal and Child Health Centres (MCHC) with maternity homes were opened one after the other with the assistance from the UNICEF and WHO. The UNICEF donated the necessary equipment for the centres while the WHO sent a team of staff to assist the development of maternity services in Hong Kong. These centres provided comprehensive maternal and child health programs including antenatal, delivery, postnatal and infant care services. A doctor supervised the care but midwives did the actual deliveries and provided immediate post-partum care. Early antenatal care was vigorously promoted and postnatal clinic was started. The general public gradually became educated about the need to have antenatal check up during pregnancy. This resulted in increased attendances at MCHCs exceeding the service capacity of the centre.
The Come of Age of Midwifery Education
Obviously, midwives were in great demand with this trend of increasing birth rate. Moreover, a number of experienced midwives had gone for private practice and set up their own maternity homes. The annual turnout of graduates from midwifery schools could not meet the needs of the hospitals. Altogether there were eight midwifery training centres at that time, namely Nethersole Hospital, Queen Mary Hospital, Kowloon Hospital, Tsan Yuk Hospital, Kwong Wah Hospital, Tung Wah Hospital, Tung Wah Eastern Hospital and Hong Kong Sanatorium and Hospital. Tsan Yuk Hospital was the centre for training of "direct entry" midwives. In early 1960s, two more midwifery training schools were opened, one at Queen Elizabeth Hospital and the other at Caritas Medical Centre.
The opening of midwifery school at Queen Elizabeth Hospital marked the beginning of midwifery training by qualified midwifery teachers. The first two tutors who possessed the qualification of "Midwifery Tutor Diploma" and taught at Queen Elizabeth Hospital were Ms Ruth Wong and the late Ms Ivy Woo.
The Static Roles of Midwives
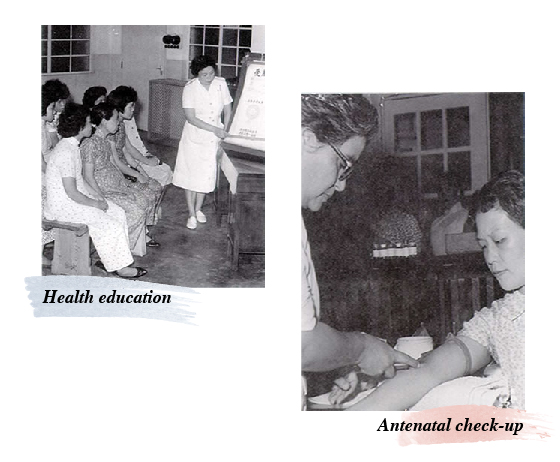
The sixties was a period of rapid development in Hong Kong, both socially and economically. During this period, the roles of midwives had basically not changed much as compared with that in the pre-war era except there was enhancement of their role in antenatal care and health education. The public became more aware of the value of disease prevention. Majority of pregnant women would attend antenatal clinic where health talks were conducted.
With better housing, water supply and sanitation, the health status of the population improved tremendously. The immunization program was also expanded and implemented with full momentum. There was marked decrease in the maternal and infant mortalities, at 42.7 per 100,000 total births and 24.9 per 1000 live births respectively in 1966.
The Splitting up of Professional Body
In 1964, the nurse members of the Nurses and Midwives Association split from the Association and formed an organization called the Nurse Associates because the nurse colleagues wanted to gain membership into the International Confederation of Nurses (ICN) and some midwife members were not registered nurses. The Association was renamed as the Hong Kong Midwives Association in 1969. The Nurse Associates became the present Hong Kong College of Nursing.
-
1970s - 1980s
PERIOD FOR MEDICAL MODEL OF CHILDBIRTH
From 1970s onwards, the practice of giving births at maternity homes gradually declined and the trend was to have hospital confinements. Women were encouraged to give birth in hospital as it was considered to be safer since medical aid could be immediately available. The notion that "birth was normal only in retrospect" had virtually discouraged any birth being taken place outside hospital, even at maternity homes which was only manned by midwives. Therefore, institutionalized childbirth became the main stream of maternity care.
Complementary Functions of Hospital and Maternity Home & Health Centre
The promotion of hospital birth and the influx of Chinese immigrants and Vietnamese boat people in the late 1970s and early 1980s posed further and immense demand on the maternity units in the hospitals. Maternity beds were always lacking even with opening of three maternity units in more hospitals, namely, Princess Margaret Hospital. Early discharge was practiced to ease the pressure on hospital beds. Women who had normal vaginal deliveries would be discharged from the maternity ward 24 to 48 hours after delivery. For those with perineal wounds and required removal of stitches, they would be transferred to the maternity homes for subsequent care.
From late 1970s onwards, the maternity homes, besides being a place for confinement for multiparous women, also served as postnatal wards housing postpartum mothers who were transferred from hospitals.
In the early eighties, there were forty-four MCHCs set up throughout the territory, easily accessible geographically to expectant mothers.
The Diminished Roles of Midwives
With the rapid advances in medical technologies and their increasing applications in maternity services such as electronic fetal monitoring, a highly technical system of childbirth was developed. Under the system in which medical science overwhelmed the maternity services, midwife became more like a technician in the hospital team. Obstetricians were in charge of all cases, both normal abnormal. The work of midwives in hospital was more like an Obstetric nurse except they personally conducted deliveries of normal cases. With the shortened stay on the postpartum ward, it was very difficult for midwives to provide proper health education on baby care and self-care, not to mention the assessment of the mothers' emotional state. Even if health education was given, it was delivered in a hasty manner. Mothers were, therefore, encouraged to take their babies to the MCHCs for care and advice.
During this two decades, maternity services was provided in a compartmentalised manner and lacked continuity of care. The roles assumed by midwives depending on the settings where they worked. For midwives working in the MCHCs, their focus of care would be more on the provision of antenatal care and health education while their colleagues in the maternity homes would conduct deliveries for normal cases and provide postnatal care. Midwives working in hospitals assumed the role of an obstetric nurse looking after both the normal and high risk pregnant/labouring women as well as the postpartum mothers. They also attended the delivery of babies. One thing in common was that, the focus of care was more on the physical aspect than the psychosocial needs of the women.
The Unification of Midwifery Training Programs
All along, there are two groups of midwives providing midwifery services, the nurse-midwives and the "direct entry" midwives. As the "direct entry" midwives had no nursing qualification, they could only work on maternity wards or the outlying maternity homes and this gave rise to staff deployment problem. As such, Tsan Yuk Hospital discontinued the training after the last intake of students in 1974. The only program that remains is the 1-year post-registration course for registered nurses.
The Decline of Maternity Homes
The success of family planning in the 80s had brought down the birth rate and also the family size. As such, less and less births took place in maternity homes. This, coupled with the adoption of medical model of childbirth, led to the declined use of maternity homes as a place for confinement. Towards the end of the decade (March 31, 1988) the last private maternity home was closed. To date, out of the nineteen public maternity homes, only three, which are all located in the outlying islands, are functioning to serve the pregnant women there in times of urgency.
-
1990s - 2000
RE-EMERGENCE OF INDEPENDENT MIDWIFERY PRACTICE
In mid 1990 the pendulum has swung back. Midwives are recognized once again as the lead professional in caring normal, low-risk pregnant women. This change was brought about by a number of factors, such as changes in the philosophy of healthcare and the infrastructure of the society, and the influence of the worldwide midwifery reform particularly that in the United Kingdom. The movement of "Changing Childbirth" in United Kingdom started in 1994. It aimed to put women and their families at the centre of maternity services, by giving mothers choice, continuity and control. Midwives have an important role in promoting services that would meet the needs of the women and their families.
The Resurrection of the Roles of Midwives
Midwife-led care is gradually re-instated. In 1993, "Midwives Clinic" was re-established in Kwong Wah Hospital. Prince of Wales Hospital introduced the "Independent Midwifery Practice" in November 1994, firstly in the delivery suite, then in the postnatal wards in 1996 and in the antenatal clinic in 1997. A full range of midwife-led services is provided to normal pregnant women from antenatal to postpartum period. Women would be referred to obstetrician only when abnormality is detected. In the following years, some form of collaborative care between obstetricians and midwives has been adopted in other obstetric units, e.g. Day Care Centre in Tsan Yuk Hospital. Currently, "Continuous Midwifery Care" is implemented in Kwong Wah Hospital. Midwives, once again, reaffirm their role in the care of normal pregnant women and healthy mothers.
Over the years, the trend of forming nuclear families has somehow deprived the young couples the social support that goes with extended families. There is no role model for the young mothers on childrearing. Parent-craft teaching is thus an important area that midwives have to address. In Hong Kong, antenatal classes run by midwives are conducted in the antenatal clinic of the obstetric units of hospitals and MCHCs. Health talks are given on the postnatal wards. There are telephone hotlines set up in the maternity units to allow mothers to seek advice from midwives on her own problem as well as the baby care.
The changing socio-economic condition in the last two decades has led to an increasing number of working women and as a result, a decline in breast feeding rate. Breast feeding promotion, therefore, becomes a priority issue for midwives. The first "Breast-feeding" clinic manned by midwives who were lactation consultants was set up in 1996 at Queen Elizabeth Hospital. Breast-feeding clinic and support groups were also formed at the MCHCs. These clinics aim to provide support, counseling and advice to nursing mothers in order to help them solve problems related to breast feeding. Nowadays, there are more than 50 midwives who are qualified as lactation consultants working in the hospitals as well as the MCHCs. According to the survey conducted by The Hong Kong Baby Friendly Hospital Initiative, the breast-feeding rate in Hong Kong has risen from 19% in 1992 to 50% in 1999, much attributed to the commitment and had work of the midwives.
The Extending Roles of Midwives
Apart from their role in the care of healthy pregnant women and normal mothers, Hong Kong midwives also work in collaboration with obstetricians in the management of women who have abnormalities and complications arising from pregnancy, childbirth and puerperium.
As childbirth is a major life event, childbirth experiences will engrave in a woman's mind for years or even a lifetime. These will have a great impact in the family life. The impact would be even greater if there is an adverse pregnancy outcome. "Bereavement Support", an area that was seldom taken note of, was first initiated in 1993 by Pamela Youde Nethersole Eastern Hospital. This service has proven to be so valuable that by now every maternity unit has its own bereavement team. Midwives are the key members of the team and they provide support and counselling to the bereaved couples to help them go through the difficult time.
Midwives also participated in the management of postnatal depression. In the Postnatal Depression Clinic at Prince of Wales Hospital, midwives are the initial care providers. They assess and counsel the at-risk women helping them to ventilate their feelings. The on-site psyciatrist would be consulted only when the woman's condition does not improve with counselling. With this kind of support, mothers with emotion problems would be managed at an early stage and thus could prevent further deterioration. The initial date from Prince of Wales Hospital did show that there was a slight decline in the number of cases referred to psychiatrist for further management.
Today's midwives have to perform a wide range of duties that are generally referred as the "enhanced roles" of midwives. They are expected not only to be proficient and competent in the technical skills, such as interpretation of cardiotocography, perineal suturing, performing ultrasonography, but also be sensitive to the emotional reaction of the women/mothers resulting from the treatments and be able to provide counselling to them, e.g. for prenatal diagnosis. Nowadays, provision of "advanced" or "specialist" clinical care is an important part of the midwives' role. In this regard, Hong Kong midwives are proactive in equipping themselves with the necessary skills and knowledge. This was clearly reflected In the ever over-subscription to related courses conducted by Hong Kong Midwives Association and other professional bodies.
Towards Professional Development
Throughout these decades, the Hong Kong Midwives Council (previously known as Hong Kong Midwives Board) works hard to improve the quality of midwifery care. All practicing midwives are recommended to take a refresher course once every five years. A midwife who has not practised for more than five years, is required to undergo a refresher course prescribed by the Council before re-commencing her practice. This helps to maintain the standard of practicing midwives and also upkeep midwifery with modern science.
In 1999, the Council has revised the Midwives Registration Ordinance in which it prohibits any person other that a registered midwife or registered medical practitioner from attending women in childbirth except those undergoing training with a view to become midwife or medical practitioner. A "Professional Development Committee" is also formed under the Council to look into the related issues. A "Code of Practice for Midwives" had been formulated by the Committee and was published by the Council in 2000. To standardize the training programs, the Council has recently issued a "core curriculum" for training of registered midwives. The curriculum enhances, among other things, the theoretical training in behavioural sciences and midwifery. The theoretical input has increased from 195 to 290 hours. From now on, any midwifery school in Hong Kong has to use this curriculum as a basis when developing its respective training program. In this way, the standard of midwifery training can be safeguarded.
Moreover, like their overseas colleagues, Hong Kong midwives are active in research studies. For the past few years, a number of studies have been conducted aiming at improving the midwifery care. Information of the studies has been disseminated in Midwifery conferences and seminars.
-
BEYONG THE 2000
MEETING THE CHALLENGES OF MIDWIFERY
The Asian Economic Crisis has left Hong Kong a drop in GPD by 5% and doubled the unemployment rate to 5.7%. With economic hardship and uncertainty, the birth rate has fallen from a plateau of around 12.0 per 1000 to 9.3 per 1000 and 8.0 per 1000 population for the past two years. The continual decrease in birth rate in the past few years has led to the merging of obstetric units in three public hospitals, namely, Caritas Medical Centre with Princess Margaret Hospital, Out Lady of Maryknoll Hospital with Kwong Wah Hospital and Tsan Yuk Hospital with Queen Mary Hospital, giving rise to a phenomenon of "surplus" midwives with the newly graduates glutted the market. In June 1999, the Head Office of Hospital Authority has "advised" all midwifery schools under its jurisdiction to suspend training for a period of two years. Currently, all midwifery schools other than that in Prince of Wales Hospital have ceased the midwifery training. This, however, can be an opportunity for changes to be made. As "quantity" decreases, the more favourable teacher-student ration in midwifery schools could improve the quality of training. Learning activities that will enhance students' skills in midwifery care such as communication and counseling and also their abilities in critical thinking and problem solving could be incorporated into the curriculum.
With the changing trend in the care of pregnant women and also higher expectation from these clients, the demand for more sophisticated maternity services is increasing. There is a need for advanced level of midwifery education. In response to this, the Chinese University of Hong Kong has started the first Masters degree programme in midwifery in 1999. Currently, there are plans to lengthen the existing basic program to an eighteen months course aiming at upgrading the midwifery education. The initial proposal has gained the support of our midwife colleagues as well as the obstetricians. If everything goes well, the upgraded midwifery program would be launched next year.
The current health care environment requires a strict control of costs while optimizing outcomes and patient/client satisfaction. One way to provide better and more coat-effective healthcare is to use skillmix more appropriately. Midwives and obstetricians have different areas of expertise and can complement each other in the delivery of maternity services. The education of midwives enables them to meet the needs of normal, healthy pregnant and birthing women as well as to detect potential problems. Obstetrician would be called in only when specialized medical knowledge or surgical skills are needed, thus freeing them to expand their horizon in obstetrics. The adoption of collaborative care would be an ideal direction for the maternity services in Hong Kong. This mode of practice fits in well with the present day healthcare policy which emphasize "value-for-money" as the full range of midwifery and obstetricians' skill are utilized.
We live in a time of rapid change and it is imperative that the change occurs in the right direction. It takes more than a hundred and fifty years for Hong Kong midwives to evolve form the ancient time of "Wan Po" to the present day of practitioner, independently taking charge of the care of women who are experiencing their normal physiological life event. Being the lead professional in the care of these women surely is a great stride that the midwifery profession in Hong Kong has made. Yet, what is more important is the quality of care that this practice has brought about: better continuity of care and more women-centred service. These are the elements of care that are highly treasured by out clients. As a midwife, ensuring every woman has a pleasant and memorable experience in childbirth, is our mission.